|
|
专业 诚信 领先
专业 诚信 领先 |
|
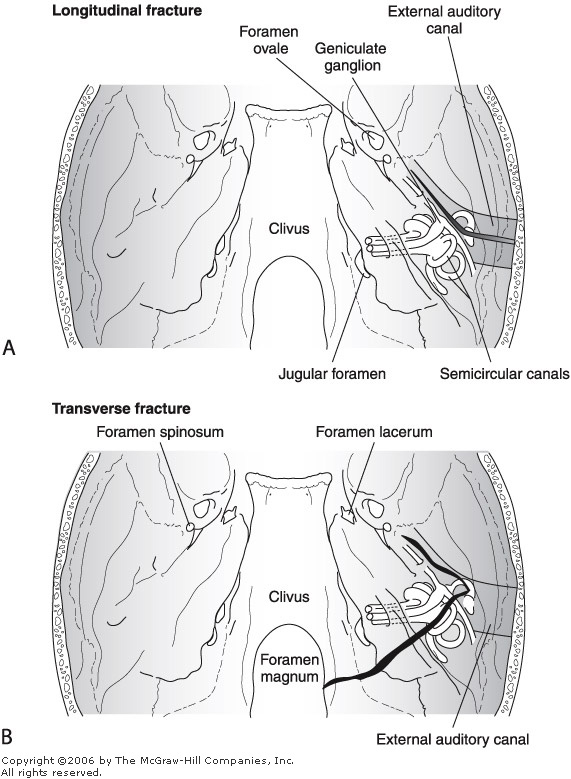
Facial Paralysis with Temporal Bone Fractures
Essentials of Diagnosis
Imaging Studies
A computed tomography (CT) scanning of the head is usually the first study performed on patients with head trauma. It is critical to rule out an intracranial hemorrhage, which may require urgent neurosurgical treatment. It is at this point that a temporal bone fracture is usually identified. High-resolution CT scanning of the temporal bone is quite valuable in delineating the extent of the fracture, CSF leak, and hemotympanum.
Facial Nerve Injury Facial nerve palsy occurs in 20% of longitudinal temporal bone fractures and 50% of transverse temporal bone fractures. The most important clinical feature to identify is whether the facial nerve palsy was of delayed or immediate onset. Patients with delayed onset palsy present to the emergency room with normal facial nerve function that slowly worsens over the next several hours to days. This is thought to represent edema within the facial nerve without disruption of neural integrity. In contrast, immediate facial nerve injury is highly suggestive of facial nerve transection. Unfortunately, it is common to have an undetermined onset time of facial nerve palsy because patients with temporal bone fractures and facial nerve palsy typically have multiple other life-threatening issues that are being dealt with at the time of the initial evaluation. These patients are often comatose and therefore quite difficult to examine.
Treatment
Usually, The treatment of delayed-onset palsy is based on conservative, nonsurgical management. But, It has a time limited, if the patient does not cure 2 month after onset, the electro-diagnostic test must be taken. patients with > 90% degeneration of neural integrity or F wave absent have been shown to have poor recovery. Presumably, the nerve is swollen within the bony fallopian canal, compressing itself within this confined space and therefore causing permanent injury to the nerve fibers. we recommend facial nerve exploration and decompression, watchful waiting is no use for these patients.
Immediate onset palsy, the surgery is need as sooner as possible. acupuncture and drugs will inevitable meet the tragic outcome.
The exploration of posttraumatic facial nerve palsy is based upon 3 routes. for more than 95% patients, A trans-mastoid sub-total decompression is enough to explore the facial nerve from the geniculate ganglion to the stylomastoid forame, even 2mm labyrinthine segment of facial nerve. For other rest 5% patient, a combined middle fossa-transmastoid facial nerve exploration is performed to delineate the facial nerve within the internal auditory canal. If the patient has a complete sensorineural hearing loss, a translabyrinthine facial nerve exploration and repair can be undertaken. This procedure allows for complete exposure of the facial nerve from the porous acousticus to the stylomastoid foramen completely through the mastoid.
Injuries are most commonly located in the area of the geniculate ganglion. If an intraneural hematoma is identified, the epineurium should be carefully opened and the hematoma evacuated. If there are bony fragments impinging upon the nerve, these can be carefully removed as well. If there is an obvious fracture of the facial nerve, the two ends of the facial nerve should be freshened and anastomosed. If the segment of missing nerve is too long to be easily anastomosed without tension, an interposition nerve graft should be utilized from the greater auricular or sural nerve. If no pathology is visualized, the act of opening the bony canal of the facial nerve should allow adequate decompression and permit swelling of the nerve without impingement. The epineurium does not need to be incised.
During the decompression, the tympanic membrane perforation will be repair and the ossicular chain dislocation (the most common form of ossicular discontinuity is incudostapedial joint dislocation) will be reconstruction. so, the presurgical conductive hearing loss will ameliorate after operation.
If you need more information, please let me konw.
Email: lijiandong@sina.com
|
|
中国面神经疾病信息网 |